VIBRANCE-MG: an ongoing study evaluating IMAAVY® + SOC in pediatric patients with antibody-positive gMG (including anti-AChR+)1


Key inclusion criteria1
- Ages 2 to <18 years
- Diagnosed with gMG, MGFA Class IIa-IVb
- Seropositive for autoantibodies (including anti-AChR)
- Suboptimal response to current stable therapy for gMG
Primary endpoints1
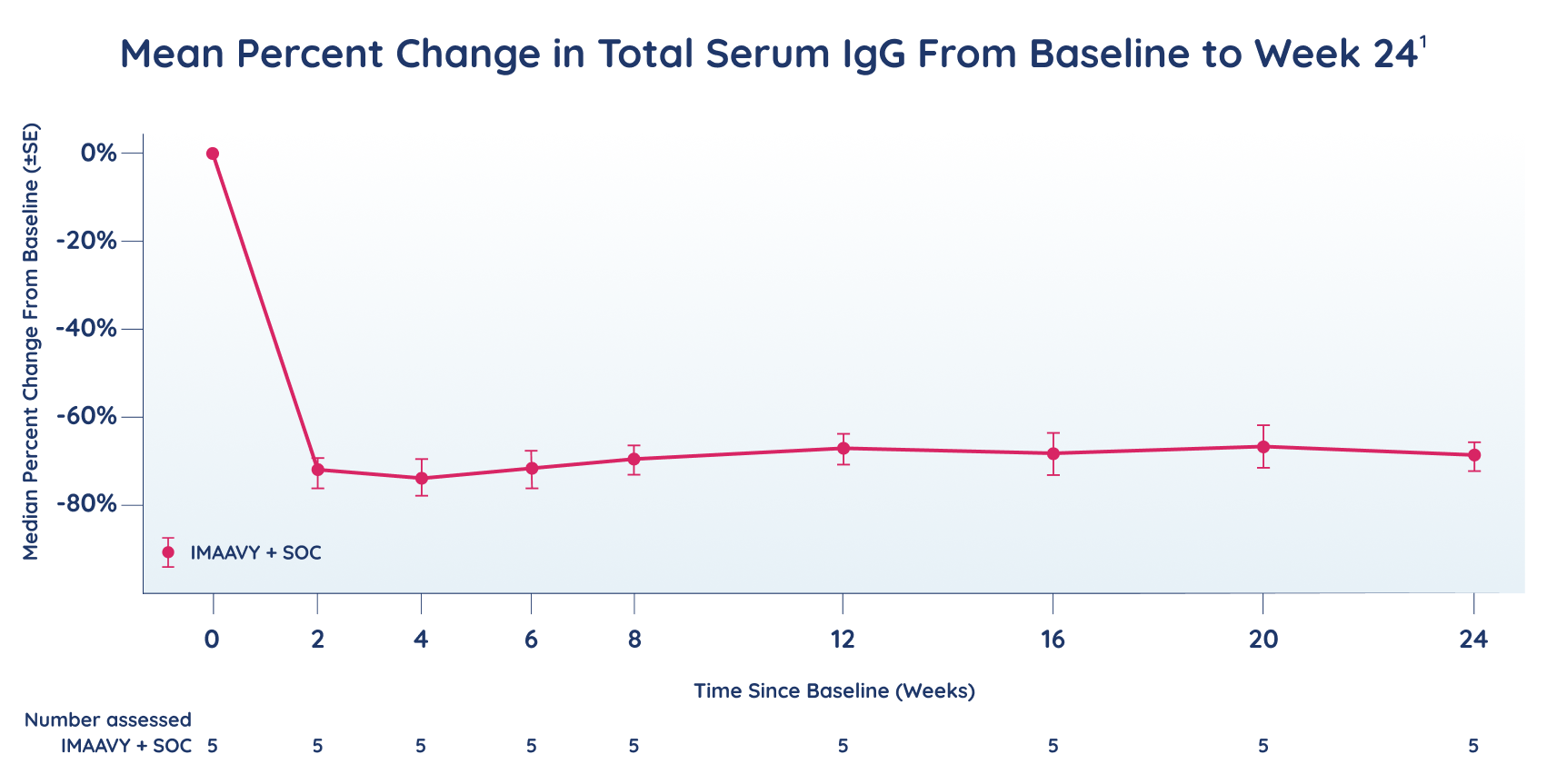
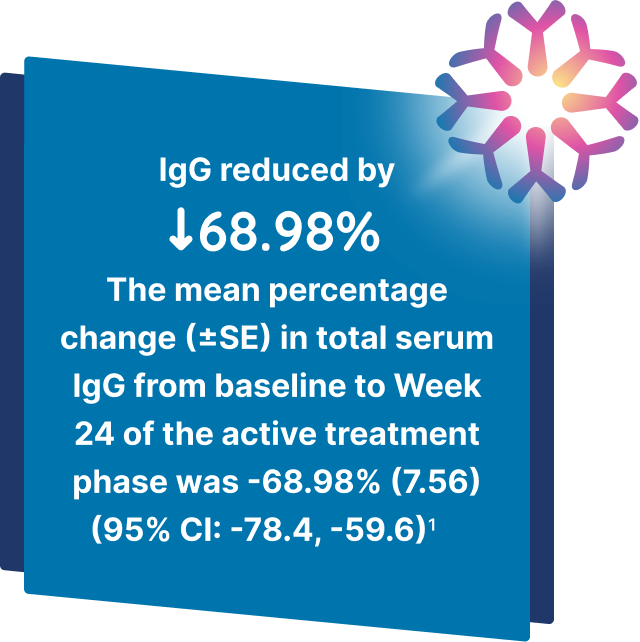
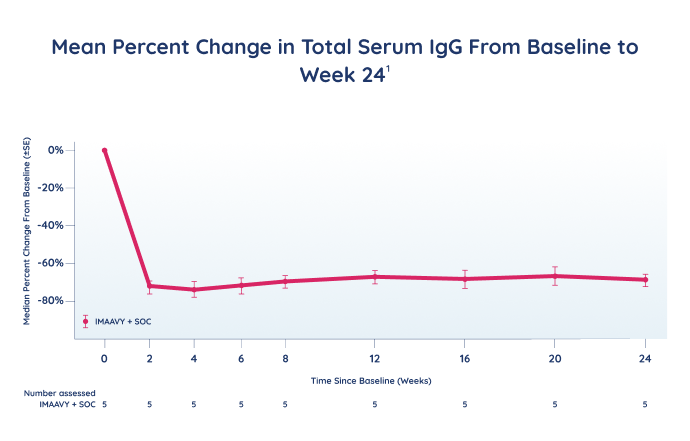
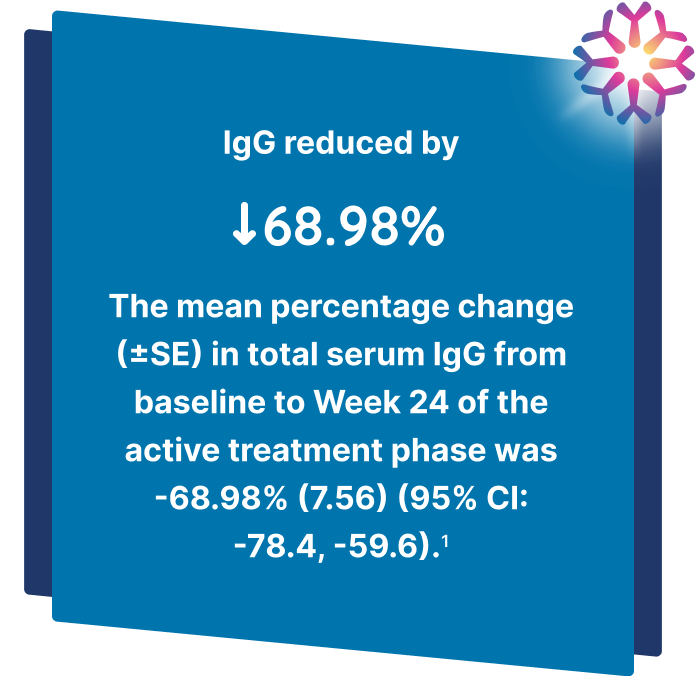
- The effect of IMAAVY + SOC on total serum IgG
- Safety and tolerability
Key secondary endpoints1
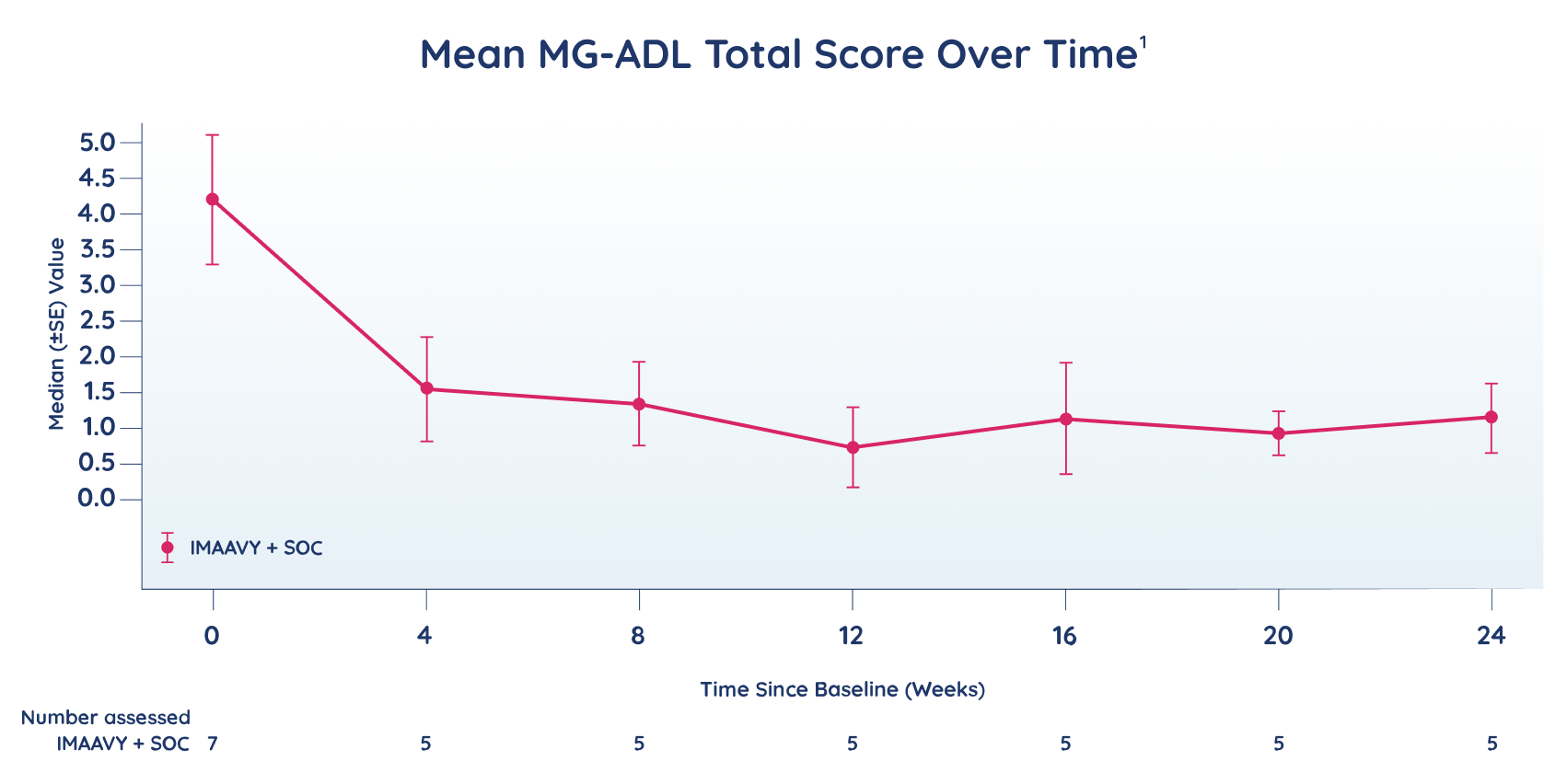
- Mean change from baseline in MG-ADL total score
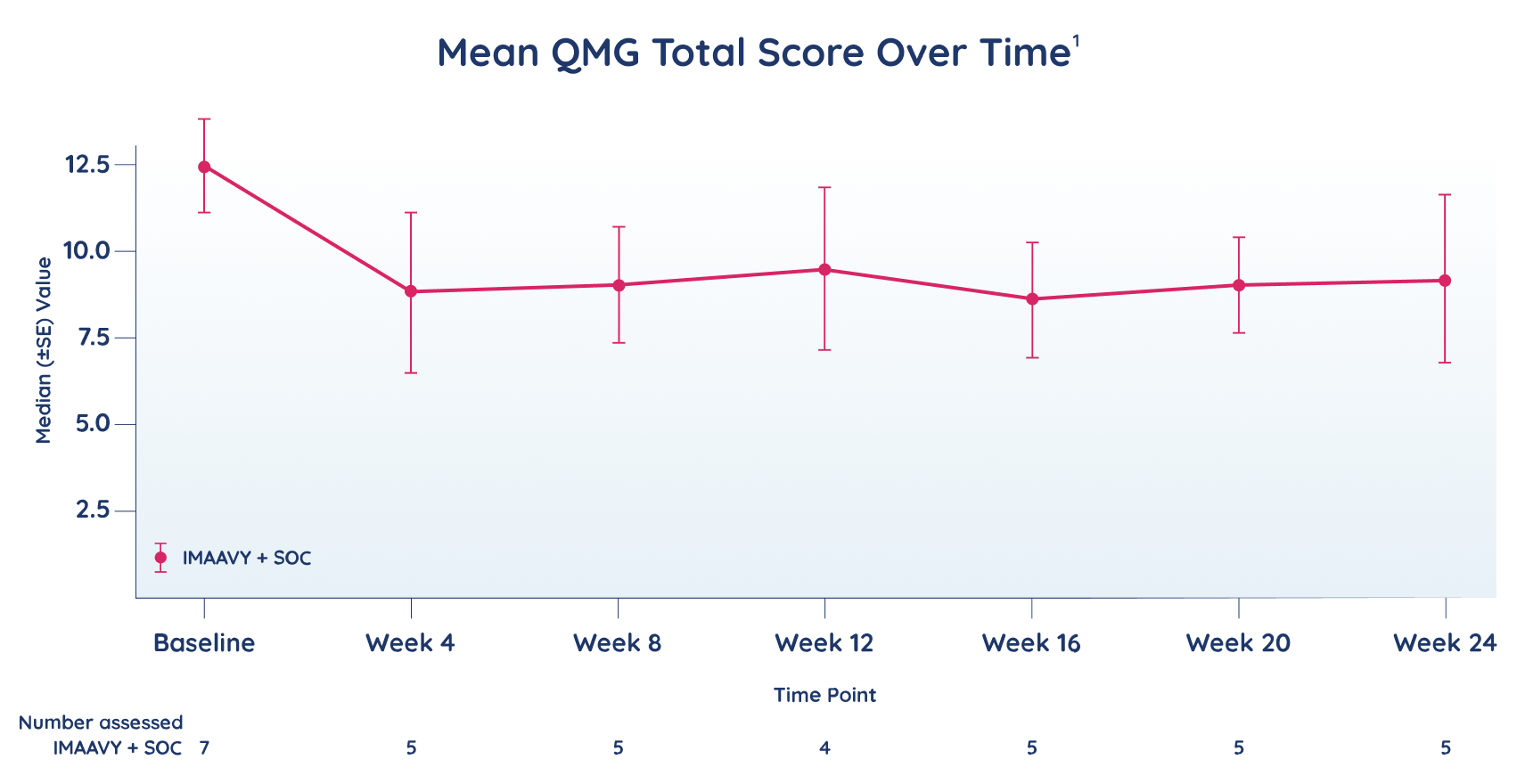
- Mean change from baseline in QMG total score
Use of IMAAVY in pediatric patients for this indication is supported by evidence from an adequate and well-controlled trial in adults with additional pharmacokinetic and safety data in pediatric patients who are 12 years of age and older.1
*30 mg/kg IV Q4W is not an approved dosing regimen for maintenance treatments; data points using this dosing were not included in the results presented.1
†Participants who withdraw or discontinue after receiving any amount of study intervention will be required to complete a safety follow-up visit 8 weeks after their last dose.1
Q2W=every 2 weeks; Q4W=every 4 weeks.
Demographics and baseline characteristics (N=7)
- Mean age = 14.1 years (range: 12-16)
- 85.7% were female
- 100% of patients were anti-AChR+
- 100% were on ≥1 concomitant MG medication‡
- At baseline, 85.7% were taking immunosuppressants, 71.4% were taking corticosteroids, and 42.9% were taking other nervous system drugs
‡SOC therapies included immunosuppressants, corticosteroids for systemic use, or other nervous system drugs.1
Limitations of this study included the open-label design, the lack of a placebo comparator, and the small sample size.
In this 24-week, single-arm study evaluating the safety of IMAAVY in 7 pediatric patients aged 12 to 16 years with gMG who were AChR+, adverse reactions were consistent with those observed in adult patients with gMG.2
| Adolescent participants N=7 | |
|---|---|
| Age, years | |
| Mean (SD) | 14.1 (1.86) |
| Range | (12; 16) |
| Sex, n (%) | |
| Female | 6 (85.7) |
| Male | 1 (14.3) |
| Race, n (%) | |
| American Indian/Alaska Native | 0 |
| Asian | 4 (57.1) |
| Black or African American | 1 (14.3) |
| White | 0 |
| Unknown | 2 (28.6) |
| Ethnicity, n (%) | |
| Hispanic or Latino | 1 (14.3) |
| Not Hispanic or Latino | 5 (71.4) |
| Unknown | 1 (14.3) |
| Weight, kg | |
| Mean (SD) | 58.19 (26.741) |
| Range | (30.9; 95.5) |
| Autoantibody type, n (%) | |
| AChR | 7 (100) |
| Baseline MG-ADL total score | |
| Mean (SD) | 4.29 (2.430) |
| Range | (2.5; 9.5) |
| Baseline QMG total score | |
| Mean (SD) | 12.50 (3.708) |
| Range | (6.5; 17.0) |
| Duration of MG, years | |
| Mean (SD) | 4.44 (3.645) |
| Range | (0.8; 11.5) |
| Age at onset of MG, years | |
| Mean (SD) | 9.70 (4.306) |
| Range | (0.5; 13.4) |
| Baseline MGFA Clinical Classification, n (%) | |
| IIa | 4 (57.1) |
| IIb | 0 |
| IIla | 2 (28.6) |
| IIlb | 1 (14.3) |
| IVa | 0 |
| IVb | 0 |
| Participants with ≥1 concomitant MG medications | 7 (100.0) |
| Immunosuppressants | 6 (85.7) |
| Corticosteroids for systemic use | 5 (71.4) |
| Other nervous system drugs§ | 3 (42.9) |
§Includes AChEIs of pyridostigmine and pyridostigmine bromide.1
AE=adverse event; SAE=serious adverse event.
References: 1. Strober J, Black S, Fitzgibbon M, et al. Safety and effectiveness of nipocalimab in adolescent participants in the open-label phase 2/3 Vibrance-MG clinical study. Poster presented at: American Association of Neuromuscular and Electrodiagnostic Medicine (AANEM) Annual Meeting; October 15-18, 2024; Savannah, GA. 2. IMAAVY [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.