VIVACITY-MG3 Phase 3 design summary1–4
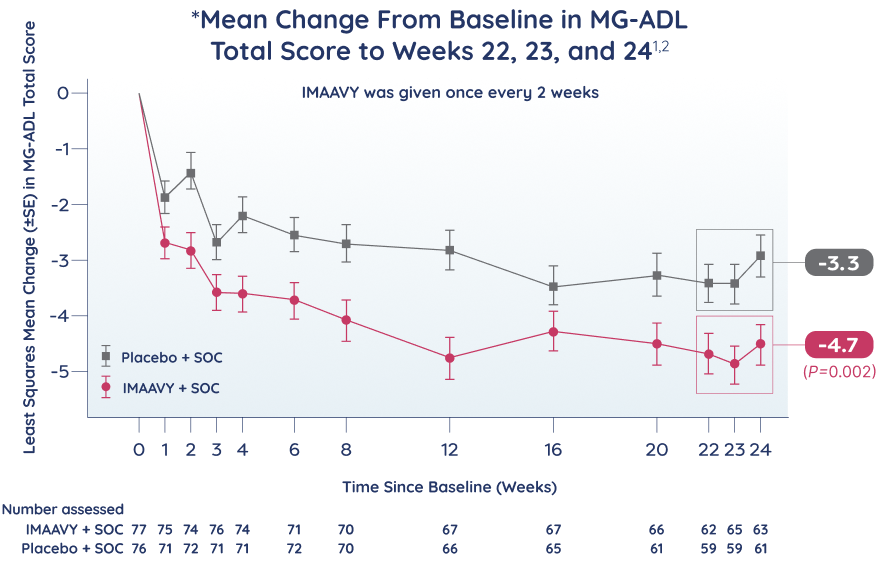
The primary endpoint for IMAAVY was evaluated to Weeks 22, 23,
and 24, which is the longest of any FcRn pivotal trial for the treatment of gMG.1,2
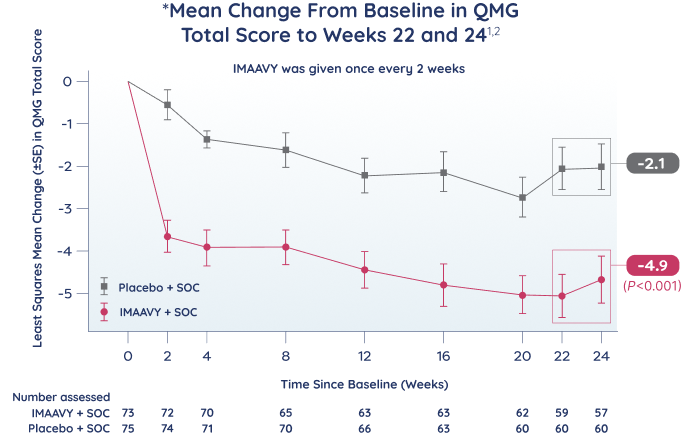
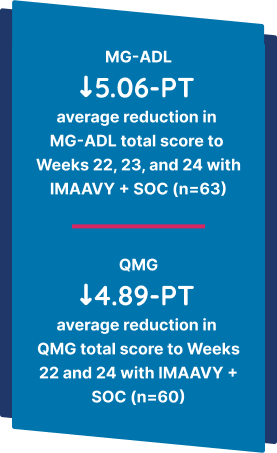
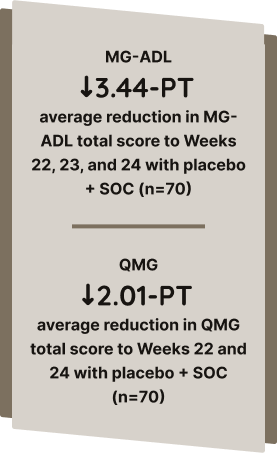
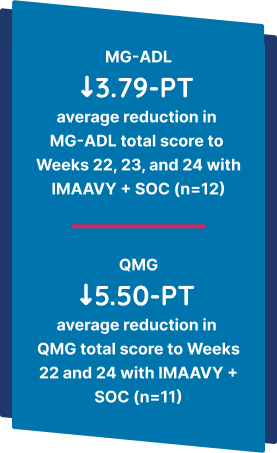
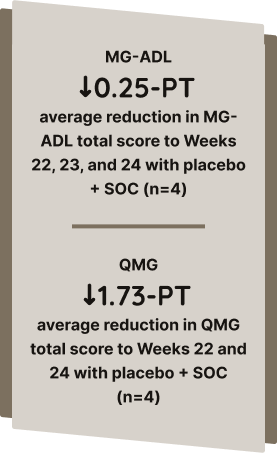
The primary efficacy endpoint was the mean change from baseline to Weeks 22, 23, and 24 in the MG-ADL total score.1


*VIVACITY is a Phase 3, multicenter, randomized, double-blind, placebo-controlled, 24-week study that assessed the efficacy and safety of IMAAVY + SOC administered via IV infusion in adult patients with gMG that was inadequately controlled (MGFA Clinical Classification Class II-IV for gMG with stable MG therapy and MG-ADL scores ≥6 at screening and baseline) vs placebo + SOC. Patients in the primary efficacy analysis set were seropositive per protocol (including anti-AChR+ or anti-MuSK+). The primary efficacy endpoint was the mean change from baseline in MG-ADL total score to Weeks 22, 23, and 24.2
†This trial included patients with the 2 most common subtypes of gMG, AChR+ and MuSK+. Eighty-eight percent (n=134) of patients were positive for anti-AChR antibodies and 10% (n=16) were positive for anti-MuSK antibodies. These subtypes account for ~90% of all patients living with gMG.1,2
‡SOC therapies included AChEIs, steroids, or NSISTs, either in combination or alone. At pivotal trial double-blind baseline, in each group, 85% of patients received AChE inhibitors, 66% of patients received steroids, and 54% of patients received NSISTs at stable doses.1
The pivotal study assessed IMAAVY + SOC therapy compared with placebo + SOC therapy. 153 antibody-positive adult patients with gMG (including anti-AChR+ or anti-MuSK+) were included in the efficacy analysis, and 196 patients were included in the safety profile analysis.1
All study participants who completed the pivotal trial period were eligible to continue into the OLE.1
Key inclusion criteria1,4:
- Adults (aged ≥18 years)
- MGFA Clinical Classification Class II a/b, III a/b, or IV a/b for gMG that was not well controlled with stable MG therapy (or for those who discontinued MG therapy due to intolerance or lack of efficacy)
- MG-ADL score ≥6 at screening and baseline
Key exclusion criteria3:
- MGFA Class I disease or presence of MG crisis (MGFA Class V)
- Certain concomitant medications or coexisting/past medical conditions (eg, hepatic, gastrointestinal, renal, pulmonary, cardiovascular, psychiatric, neurological or musculoskeletal disorder, hypertension)
- Infections/immunodeficiency
- Patients who are lactating or pregnant
- Other (hypersensitivity to IMAAVY, suicidal ideation, severe substance or alcohol use disorder, etc)
| IMAAVY + SOC | Placebo + SOC | Total | |
|---|---|---|---|
| N | |||
| N | 77 | 76 | 153 |
| Age | |||
| Mean years (SD) | |||
| Mean years (SD) | 52.5 (15.66) | 52.3 (16.37) | 52.4 (15.97) |
| Range | |||
| Range | 20-81 | 20-81 | 20-81 |
| Sex, n (%) | |||
| Female | |||
| Female | 50 (65%) | 42 (55%) | 92 (60%) |
| Male | |||
| Male | 27 (35%) | 34 (45%) | 61 (40%) |
| Race, n (%) | |||
| American Indian or Alaska Native | |||
| American Indian or Alaska Native | 1 (1%) | 0 | 1 (1%) |
| Asian | |||
| Asian | 24 (31%) | 25 (33%) | 49 (32%) |
| Black or African American | |||
| Black or African American | 1 (1%) | 1 (1%) | 2 (1%) |
| White | |||
| White | 49 (64%) | 47 (62%) | 96 (63%) |
| Not reported | |||
| Not reported | 2 (3%) | 3 (4%) | 5 (4%) |
| Antibody status at screening | |||
| N | |||
| N | 77 | 76 | 153 |
| Seropositive, n (%)§ | |||
| Seropositive, n (%)§ | 77 (100%) | 76 (100%) | 153 (100%) |
| Anti-AChR+, n (%) | |||
| Anti-AChR+, n (%) | 63 (82%) | 71 (93%) | 134 (88%) |
| Anti-MuSK+, n (%) | |||
| Anti-MuSK+, n (%) | 12 (16%) | 4 (5%) | 16 (10%) |
| Baseline MG-ADL score | |||
| N | |||
| N | 77 | 76 | 153 |
| Mean (SD) | |||
| Mean (SD) | 9.4 (2.73) | 9.0 (1.97) | 9.2 (2.38) |
| Range | |||
| Range | 6–18 | 6–13 | 6–18 |
| ≤9, n (%) | |||
| ≤9, n (%) | 48 (62%) | 45 (59%) | 93 (61%) |
| >9, n (%) | |||
| >9, n (%) | 29 (38%) | 31 (41%) | 60 (39%) |
| Baseline QMG score | |||
| N | |||
| N | 77 | 76 | 149 |
| Mean (SD) | |||
| Mean (SD) | 15.1 (4.78) | 15.7 (4.92) | 15.4 (4.85) |
| Range | |||
| Range | 7-28 | 5-28 | 5-28 |
| MGFA class | |||
| N | |||
| N | 77 | 76 | 153 |
| I, n (%) | |||
| I, n (%) | 1 (1%)|| | 0 | 1 (1%) |
| lla, n (%) | |||
| lla, n (%) | 7 (9%) | 10 (13%) | 17 (11%) |
| llb, n (%) | |||
| llb, n (%) | 11 (14%) | 10 (13%) | 21 (14%) |
| llla, n (%) | |||
| llla, n (%) | 34 (44%) | 29 (38%) | 63 (41%) |
| lllb, n (%) | |||
| lllb, n (%) | 17 (22%) | 15 (20%) | 32 (21%) |
| lVa, n (%) | |||
| lVa, n (%) | 3 (4%) | 10 (13%) | 13 (9%) |
| lVb, n (%) | |||
| lVb, n (%) | 4 (5%) | 2 (3%) | 6 (4%) |
AChEI=acetylcholinesterase inhibitor; AChR=acetylcholine receptor; AE=adverse event; DB=double blind; FcRn=neonatal fragment crystallizable receptor; gMG=generalized myasthenia gravis; IV=intravenous; MACE=major adverse cardiovascular event; MG=myasthenia gravis; MG-ADL=Myasthenia Gravis Activities of Daily Living; MGFA=Myasthenia Gravis Foundation of America; MOA=mechanism of action; MuSK=muscle-specific tyrosine kinase; NSIST=non-steroidal immunosuppressive therapy; OLE=open-label extension; Q2W=every 2 weeks; QMG=Quantitative Myasthenia Gravis; SD=standard deviation; SE=standard error; SOC, standard of care.
§Eighty-eight percent (n=134) of patients were positive for AChR antibodies and 10% (n=16) were positive for MuSK antibodies. These subtypes account for ~90% of all patients living with gMG.1,2
||Patient had MGFA Class IIa at screening and MG-ADL of 8 at both screening and baseline.
References: 1. IMAAVY [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc. 2. Antozzi C, Vu T, Ramchandren S, et al. Safety and efficacy of nipocalimab in adults with generalised myasthenia gravis (Vivacity-MG3): a phase 3, randomised, double-blind, placebo-controlled study. Lancet Neurol. 2025;24(2):105–116. doi:10.1016/S1474-4422(24)00498-8 3. Data on file. Janssen Biotech, Inc. 4. Antozzi C, Vu T, Ramchandren S, et al. Supplement to: Safety and efficacy of nipocalimab in adults with generalised myasthenia gravis (Vivacity-MG3): a phase 3, randomised, double-blind, placebo-controlled study. Lancet Neurol. 2025;24(2):105–116. doi:10.1016/S14N4-4422(24)00498-8